Professional Corn & Callus Debridement
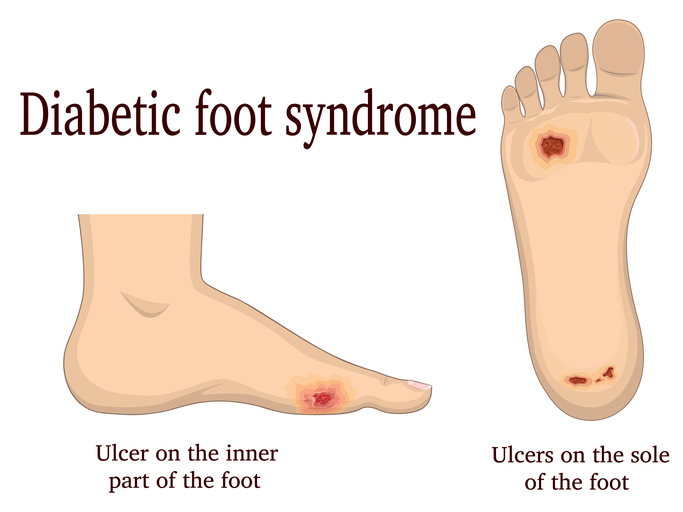
Corns and calluses, also known as hyperkeratotic lesions, affect most of us. In some cases, they can become problematic, leading to uncomfortable pressure points or even ulcerations in diabetic patients.
The treatment for hyperkeratotic lesions is regular debridement. With proper debridement, a patient can remain comfortable for 60-90 days in between treatments.
Other modifications include appropriate shoes and aperture padding such as Dr. Scholl's pads. When hyperkeratotic lesions are the result of a hammertoe or a bunion, surgical modification may be considered. However, not everyone will be a surgical candidate and only a doctor should decide when surgery is appropriate.
It's important to be able to identify corns and calluses appropriately, and to judge whether or not they should be immediately addressed to avoid future pressure points and subsequent ulcerations.
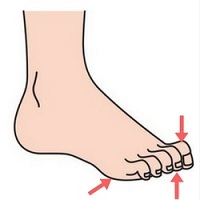 Hammertoes are one of the leading musculoskeletal causes for hyperkeratotic lesions. A hammertoe is a contracted digit and can have more than one pressure point. Lesions can occur under the metatarsal head, on the top of the toe and at the distal tip of the toe. Since the distal tip of a toe does not have much padding, these types of lesions are very common and very painful.
When examining the foot, we must look at all three potential spots to identify the potential for lesions. Additionally, briefly examine the skin on order to identify signs of arterial insufficiency, another risk factor for lesions. As a foot care nurse, it's vital to be able identify a high-risk person in seconds in order to have a better idea of an appropriate treatment plan. Hammertoes are one of the leading musculoskeletal causes for hyperkeratotic lesions. A hammertoe is a contracted digit and can have more than one pressure point. Lesions can occur under the metatarsal head, on the top of the toe and at the distal tip of the toe. Since the distal tip of a toe does not have much padding, these types of lesions are very common and very painful.
When examining the foot, we must look at all three potential spots to identify the potential for lesions. Additionally, briefly examine the skin on order to identify signs of arterial insufficiency, another risk factor for lesions. As a foot care nurse, it's vital to be able identify a high-risk person in seconds in order to have a better idea of an appropriate treatment plan.
It’s common to find lesions associated with the plantar heads on the plantar surface of the foot. This area is easy to debride either with a sander or with a scalpel. Debridement here is important because an ulceration can occur underneath the hyperkeratotic buildup, where it could easily go unnoticed.
Upon sanding, it's not entirely uncommon to discover discoloration. If this occurs, your patient should know about what you've uncovered before you continue.
Sharp Debridement
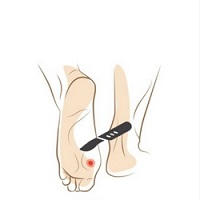 Sharp debridement falls within most nurses’ scope of practice, however, it's best to check individual state and facility regulations regarding this. Sharp debridement is the fastest way to eliminate the pressure that a callus causes, and is done simply by removing hyperkeratotic tissue from the top of the skin.
In order to avoid exposure of the patient's most sensitive skin, always leave a small portion of the callus when debriding or sanding. Sharp debridement falls within most nurses’ scope of practice, however, it's best to check individual state and facility regulations regarding this. Sharp debridement is the fastest way to eliminate the pressure that a callus causes, and is done simply by removing hyperkeratotic tissue from the top of the skin.
In order to avoid exposure of the patient's most sensitive skin, always leave a small portion of the callus when debriding or sanding.
Sanding
The Dremel drill is the quickest and easiest way to sand, although it does create fine dust  particles which can be inhaled and cause subsequent allergic reactions. While allergies and reactions such as asthma can be triggered, note that there is no literature that documents pulmonary fungal infection as a result of inhaling dust from calluses. particles which can be inhaled and cause subsequent allergic reactions. While allergies and reactions such as asthma can be triggered, note that there is no literature that documents pulmonary fungal infection as a result of inhaling dust from calluses.
 Once a callus has been debrided, either sharply or with the Dremel, it's important to pad the foot so that so the patient is more comfortable and the callus does not come back as quickly. A buttress pad, also known as a crest pad, is designed to relieve distal tip pressure. Buttress pads are available in leather or silicone, and can easily be made at home with round dental gauze. The general idea, no matter the material, is that the toes become pushed upward to avoid walking on the distal tip. This prevents pain and ulcerations. We at Rainier Medical Education have a great following of patients who love these and wear them consistently. Once a callus has been debrided, either sharply or with the Dremel, it's important to pad the foot so that so the patient is more comfortable and the callus does not come back as quickly. A buttress pad, also known as a crest pad, is designed to relieve distal tip pressure. Buttress pads are available in leather or silicone, and can easily be made at home with round dental gauze. The general idea, no matter the material, is that the toes become pushed upward to avoid walking on the distal tip. This prevents pain and ulcerations. We at Rainier Medical Education have a great following of patients who love these and wear them consistently.
How long should a buttress pad be worn?
Since a pad used for foot correction does not fix the underlying problem, without surgical intervention, a foot pad will need to be worn for life.
Aperture pads are available in most stores and come in medicated and un-medicated varieties. For patient safety, it is vital that the pad used is un-medicated.
The hole in the aperture pad should be large enough to go around the entire lesion with a little room left over. If the hole is too small, it's alright to cut or stretch it. Aperture pads can be worn with hammertoes, and secured with a Band-Aid for longer wear. Generally, the adhesive backing on an aperture pad also protects the skin from moisture.
Other forefoot pads that are readily available in stores and online include hammertoe pads. Ideal hammertoe pads offer a toe loop to go over one of the toes while the comfort pad sits securely underneath. A product like this is effective in padding plantar forefoot lesions, as well as controlling hammertoes.
Pressure-relief pads within the shoe can be professionally made to accommodate a lesion with cut-outs in the orthotic, while extra-depth shoes will accommodate such inserts as well as hammertoes. A comfortable tennis shoe can act as a very affordable extra-depth shoe. The insole can be easily removed and replaced.
Modifying existing shoe gear can accomplish similar results. If your patient has obvious signs of shoe wear indicating hammertoes or bunions, mark them with masking tape to have them taken to the shoe repair technician to stretch those spots out.
We do not recommend using an at-home shoe-stretching device since these tend not to work properly.
 Since your patients likely won't be able to visit you as often as we'd like, patient education pieces like the one above are a great way to encourage healthy feet at home. Since your patients likely won't be able to visit you as often as we'd like, patient education pieces like the one above are a great way to encourage healthy feet at home.
If your patient has thick and well-nourished skin, we recommend a sanding paddle or a PedEgg between visits as well as wearing appropriately fitting footwear.
Under no circumstances should patients ever Dr. Scholl's corn remover liquids, which contain acids not specific to hyperkeratotic tissue. Products like these will dissolve all skin and are often used improperly, with tragic results.
Additionally, these products do not remove corns or calluses, but simply soften them, leaving the underlying problem intact.
Hyperkeratotic tissue can be sanded or sharply debrided, then further cared for with proper pads, shoes or shoe inserts. By educating our patients and providing regular care, the foot care nurse can prevent ongoing pain, lesions and ulcerations.
|
|
|

 Directed by
Directed by Podiatric Physician
Podiatric Physician Wound Care
Wound Care High Risk Foot
High Risk Foot